

As Covid-19 vaccine passes become part of life for most New Zealanders, Naomii Seah talks to expert Dr Heather Battles about their historical precedents, and what we can learn from past health responses in Aotearoa.
“This is not some unprecedented, radically new thing,” says Dr Heather Battles.
Battles, a lecturer of anthropology and social sciences at the University of Auckland who specialises in the history of epidemics and pandemics, is speaking about the Covid-19 vaccine pass system, which came into effect last week when New Zealand moved into the traffic light system. Under the new system, New Zealanders have to show their passes at places like hospitality venues, gyms and other close-contact businesses – but not essential services – in order to return to a “new normal”.
As Battles acknowledges above, the pass system is one in a long line of pandemic responses across history, including controlling borders, nationwide lockdowns and vaccinations.

She notes that infection control measures vary widely over time periods and areas, but that health certificates, immunity passports and vaccine passports could all be considered related measures. That is, they are all systems of documentation that restrict access between areas as epidemics unfold.
Perhaps one of the earliest such systems was the implementation of quarantine regulations in England during 1664 to combat the plague. No ships could leave Turkey or Egypt without a bill of health, which couldn’t be issued unless 40 days had passed without an instance of plague at the port of departure.
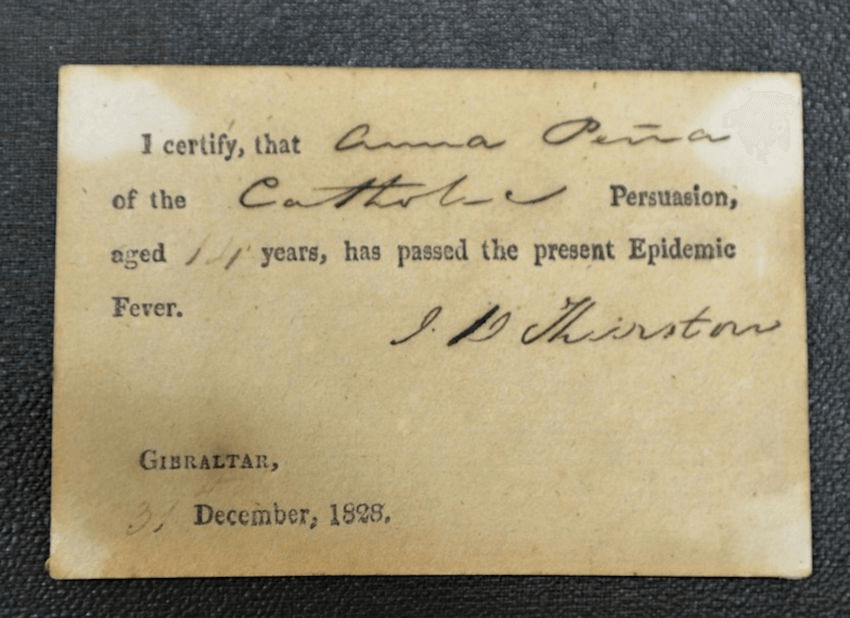
Another recently discovered early system is the “fever passes” of 1828, implemented during a yellow fever outbreak in Gibraltar. An encampment was built to forcibly quarantine those who were ill. The combination of fever passes and quarantine measures was somewhat successful in controlling the outbreak; mortality in Gibraltar dropped to 19.75 per 1,000, while elsewhere it was 103.90 per 1,000.
At the end of the 19th century, continuing into the 20th, a series of “International Sanitary Conferences” were held. These aimed to develop policies around controlling infection, which became more urgent as air travel became cheap and commercially available.
One such convention, the International Sanitary Convention for Aerial Navigation, held in 1933 in Paris, was signed by 66 countries, including New Zealand. It contained specific policies to prevent the spread of cholera, yellow fever, plague, typhus and smallpox. Among these policies, vaccination (then known as “inoculation”) certificates were proposed for cholera, smallpox and yellow fever.
In 1980, smallpox was declared eradicated by the World Health Organisation. This was attributed to the high rates of smallpox vaccination, encouraged in part by the mandatory smallpox vaccinations required for travel.
In the modern day, yellow fever vaccination is still mandatory to enter some high-risk countries. The International Certificate of Vaccination of Prophylaxis has been in use (in some form) since 1933.
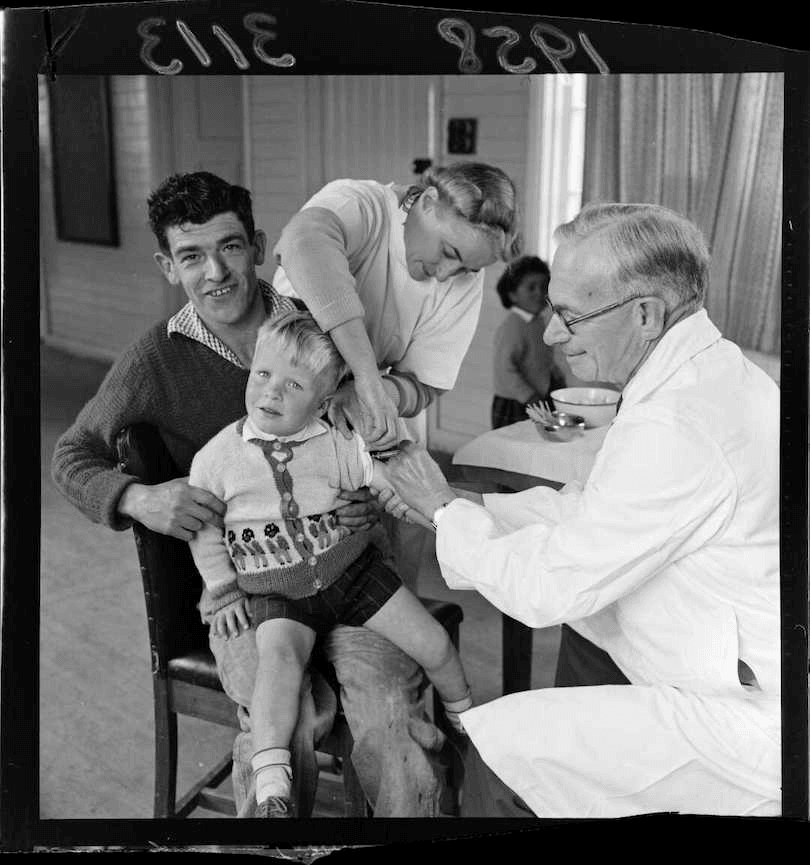
There’s also a local precedent for vaccine mandates. In 1863, vaccination of children against smallpox was mandatory, and remained so until the early 20th century. Although not mandated, the polio vaccine was given to all children in schools from 1956, and by 1959, the vast majority of children aged two to 16 in the country had been vaccinated against polio.
Before the vaccine was developed, in the polio outbreaks of the 1940s, schools were shut and health certificates were employed to allow children to travel between restricted areas.
These systems do work for infection control; they’re established measures that have worked in the past. In particular, vaccine passes can encourage vaccination and control infection. But as always, these benefits come at a cost.
“What epidemics do is they make the inequalities that exist visible,” notes Battles. “They reveal the fault lines of society.”
And in New Zealand, these fault lines often run straight through our Māori, low-socioeconomic and minority communities.
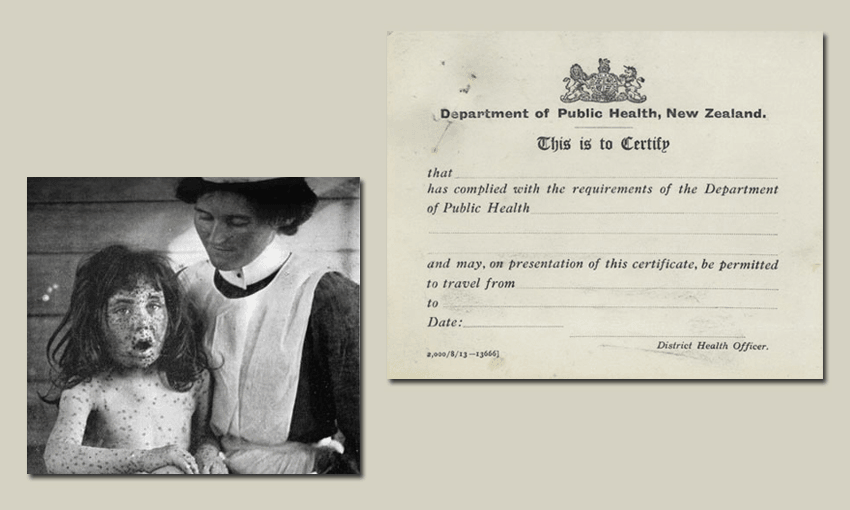
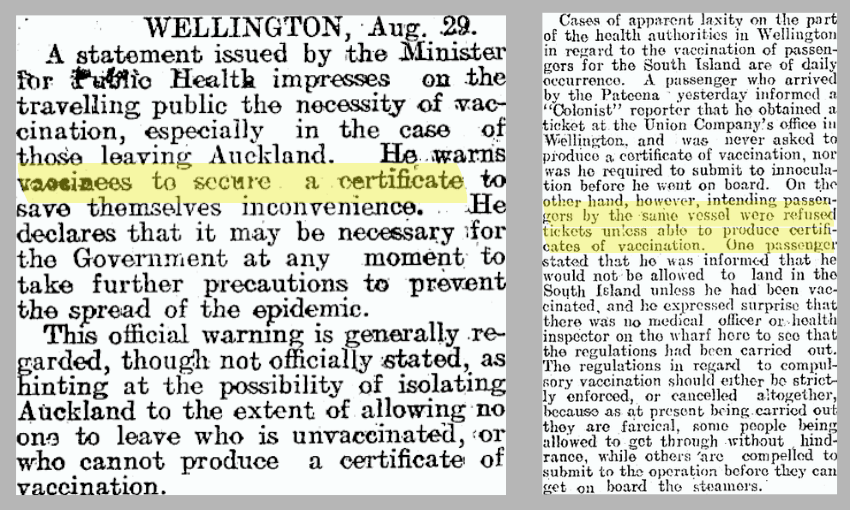
During the 1913 smallpox epidemic in New Zealand, governments imposed harsh quarantines and travel restrictions on Māori communities. Medical treatment was limited, and food was in short supply. A vaccinated group of Māori who sought help in Hamilton were turned away by Mayor Manning, who later passed a motion to ban Māori completely.
Vaccination certificates were a requirement for Māori travellers, though some Māori, as in the Hamilton case, were still turned away. To access a vaccine, many had to travel into towns, but travel into towns was banned without a vaccine certificate. Pākehā were prioritised for vaccinations, although Māori were the highest-risk population. The combination of poor medical access, poor nutrition, poor infrastructure, racism and inadequate social support led to a death toll of 55, all of them Māori.
At the time, compulsory vaccination was also described as “severe class legislation” in the Ohinemuri Gazette. In a letter to the editor, a member of the public expressed concern that those with resources and power would escape notice, while the vulnerable would be subject to persecution.
These historical inequities are reflected in today’s pandemic situation. Battles notes that not everyone has access to a smartphone. Those without smartphones will likely require a physical vaccine pass, which will require ID checks. Many of our vulnerable people don’t have appropriate IDs. Then there’s access to the vaccine. In remote areas, driving to a vaccination centre could take hours. And those living in rural areas may have indirect access issues too, such as limited options for vehicle repair and registration.
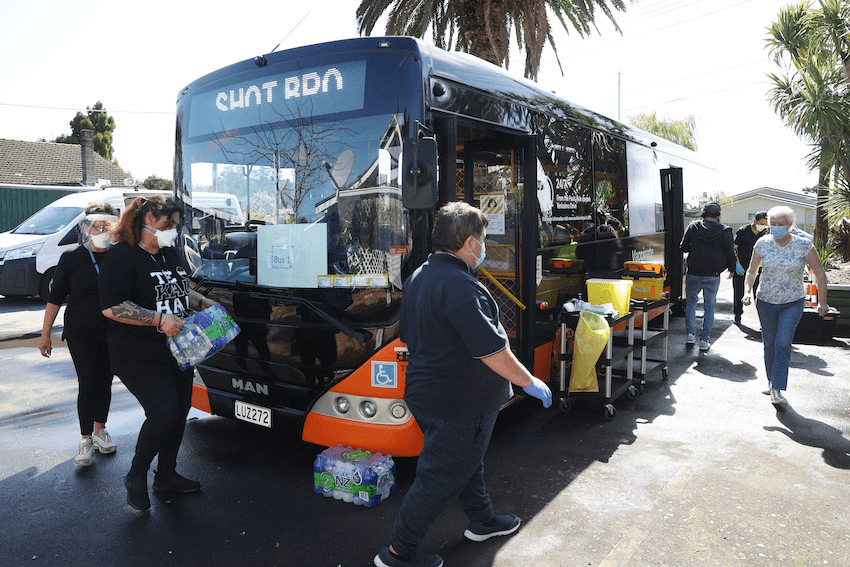
The good news is that public health interventions – such as vaccine buses and vans, public vaccination campaigns, and community outreach programmes – are being reflected in our increasing vaccination rates. Then again, worldwide vaccine shortages are also having an impact. Paediatric vaccines, for example, are still unavailable, and some communities simply have a much higher proportion of young people.
But New Zealand is at an advantage, both with the vaccine pass system and the wider health response to Covid-19. As we’ve been relatively Covid free, Battles says it’s important to look both overseas and to history to learn how to strengthen our systems.
“A lot of this is predictable,” says Battles. “None of it is a big mystery.
“Strengthening basic healthcare systems, strengthening basic community care, improving health equality and population health in general is the best thing, because you don’t have these huge vulnerabilities just sitting there.
“With Covid,” she adds, “a lot of mortality comes from people with so-called underlying conditions.”
She cites the ongoing battle with rheumatic fever in South Auckland, which has been linked to poor housing conditions. “Improving living conditions and improving inequalities and things like that, you’d be in a much better position with Covid.
“Epidemics happen and you have to respond with emergency measures, but how those measures impact people, and whether they exacerbate existing inequalities, depends on the situation already.”